
How the CDC Abandoned Science
Mass youth hospitalizations, COVID-induced diabetes, and other myths from the brave new world of science as political propaganda
February 15, 2022

The main federal agency guiding America’s pandemic policy is the U.S. Centers for Disease Control, which sets widely adopted policies on masking, vaccination, distancing, and other mitigation efforts to slow the spread of COVID and ensure the virus is less morbid when it leads to infection. The CDC is, in part, a scientific agency—they use facts and principles of science to guide policy—but they are also fundamentally a political agency: The director is appointed by the president of the United States, and the CDC’s guidance often balances public health and welfare with other priorities of the executive branch.
Throughout this pandemic, the CDC has been a poor steward of that balance, pushing a series of scientific results that are severely deficient. This research is plagued with classic errors and biases, and does not support the press-released conclusions that often follow. In all cases, the papers are uniquely timed to further political goals and objectives; as such, these papers appear more as propaganda than as science. The CDC’s use of this technique has severely damaged their reputation and helped lead to a growing divide in trust in science by political party. Science now risks entering a death spiral in which it will increasingly fragment into subsidiary verticals of political parties. As a society, we cannot afford to allow this to occur. Impartial, honest appraisal is needed now more than ever, but it is unclear how we can achieve it.
In November 2020, a CDC study sought to prove that mask mandates slowed the spread of the coronavirus. The study found that counties in Kansas which implemented mask mandates saw COVID case rates start to fall (light blue below), while counties that did not saw rates continue to climb (dark blue):
The data scientist Youyang Gu immediately noted that locales with more rapid rise would be more likely to implement a mandate, and thus one would expect cases to fall more in such locations independent of masking, as people’s behavior naturally changes when risk escalates. Gu zoomed out on the same data and considered a longer horizon, and the results were enlightening: It appeared as if all counties did the same whether they masked or not:
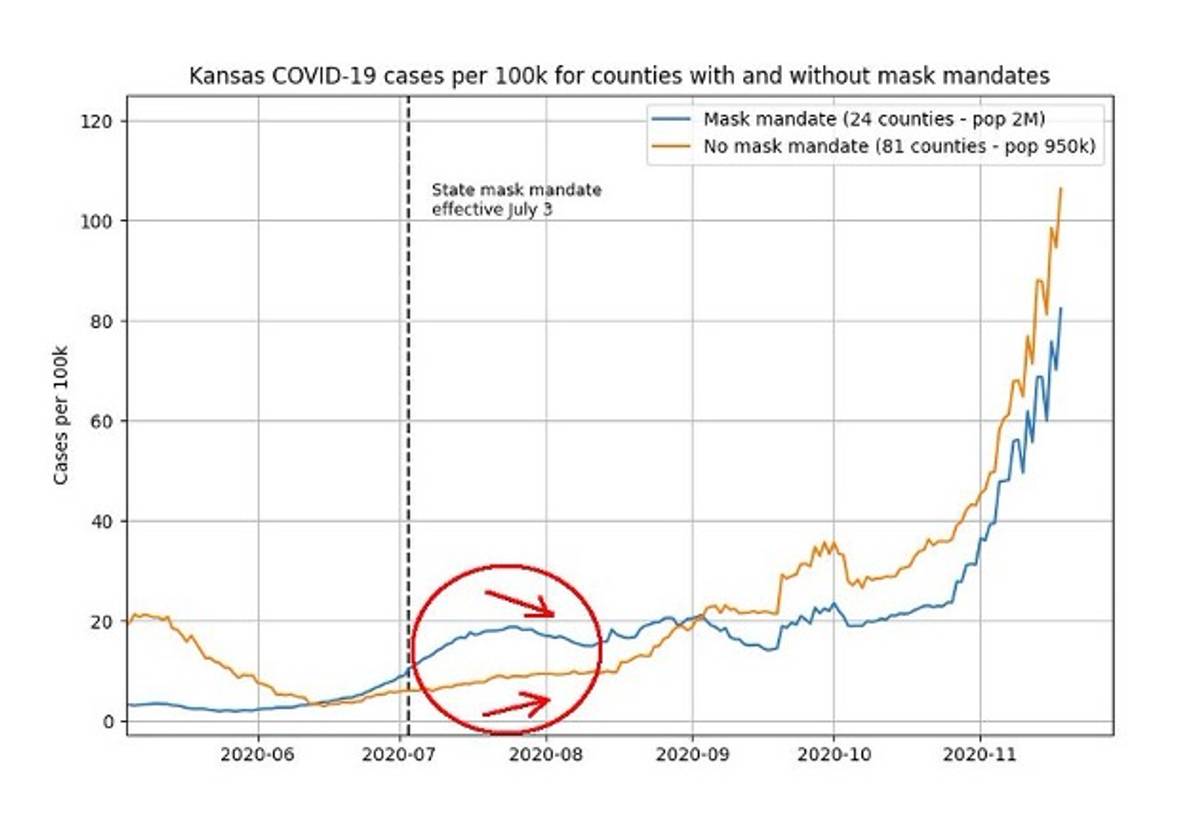
The CDC had merely shown a tiny favorable section, depicted in the red circle above, but the subsequent pandemic waves dwarf their results. In short, the CDC’s study was not capable of proving anything and was highly misleading, but it served the policy goal of encouraging cloth mask mandates.
When it comes to promoting mask mandates in school, in October 2021 the CDC famously offered a comparison of masked and unmasked schools in Arizona’s Pima and Maricopa counties in their own journal, Morbidity and Mortality Weekly Report (MMWR). The analysis claimed that schools with no mask requirement were 3.5 times more likely to experience a COVID outbreak when compared with schools that mandated masking. But the analysis did not adjust for rates of vaccination among either teachers or students. The paper also looked at two counties in Arizona with different political preferences, and thus did not separate mask mandates from other patterns of behavior that fall within partisan lines. Democratic voters, for example, are much more likely to embrace mask mandates and are more likely to otherwise curtail their behavior as they report greater overall concern about COVID. Elementary schoolchildren generally do better with COVID than high school kids, but the CDC’s analysis lumped all ages together, and might have been biased by the fact that mask mandates were more common at ages when outbreak detection occurs less often.
These were only a few of the CDC paper’s problems. When the reporter David Zweig investigated it for The Atlantic, he found that the exposure times varied: The mask mandate schools were open for fewer hours per day, with less time for outbreaks to occur. Zweig also found that the number of schools included did not add up. He hypothesized that some schools conducting remote learning might have been wrongly included, but when he asked the paper’s authors to provide him a list of the schools, they didn’t. In short, the more one examined this study, the more it fell apart.
Masking is not the only matter in which the CDC’s stated policy goal has coincided with very poor-quality science that was, coincidentally, published in their own journal. Consider the case of vaccination for kids between the ages of 5 and 11. COVID vaccination in this age group has stalled, which runs counter to the CDC’s goal of maximum vaccination. Interestingly, vaccinating kids between 5 and 11 is disputed globally; Sweden recently elected not to vaccinate healthy kids in this age group, and some public health experts believe that it would be preferable for kids to gain immunity from natural exposure instead. Stalling U.S. uptake therefore reflects a legitimate and open scientific debate, regardless of whether the CDC’s policy goal would like to consider it closed.
Enter the CDC’s new study. Widely covered in news outlets, the January 2022 study claims that kids below the age of 18 who get diagnosed with COVID are 2.5 times more likely to be diagnosed with diabetes. “These findings underscore the importance of COVID-19 prevention among all age groups,” the authors write, “including vaccination for all eligible children and adolescents.” But a closer examination of the study again reveals problems.
First, it does not adjust for body mass index. Higher BMI is a risk factor for COVID, prompting hospitalization and diabetes, and yet the CDC analysis does not adjust for weight at all. Second, the absolute risks the study finds are incredibly low. Even if the authors’ finding is true, it demonstrates an increase in diabetes of up to 6 in 10,000 COVID survivors. Third, the CDC’s analysis uses billing record diagnoses as a surrogate for COVID cases, but many kids had and recovered from COVID without seeking medical care. Without a true denominator that conveys the actual number of COVID cases, the entire analysis might be artifact. As the former dean of Harvard Medical School Jeffrey Flier told The New York Times, “The CDC erred in taking a preliminary and potentially erroneous association and tweeting it to specifically create alarm in parents.” Some might view it as a mistake, but after observing these matters for almost two years, I believe it was the entire point of the study: Alarm might boost flagging vaccine uptake in kids. (Already, a better study out of the United Kingdom finds no causal link between COVID and diabetes in kids.)
Some might view it as a mistake, but I believe it was the entire point of the study: Alarm might boost flagging vaccine uptake in kids.
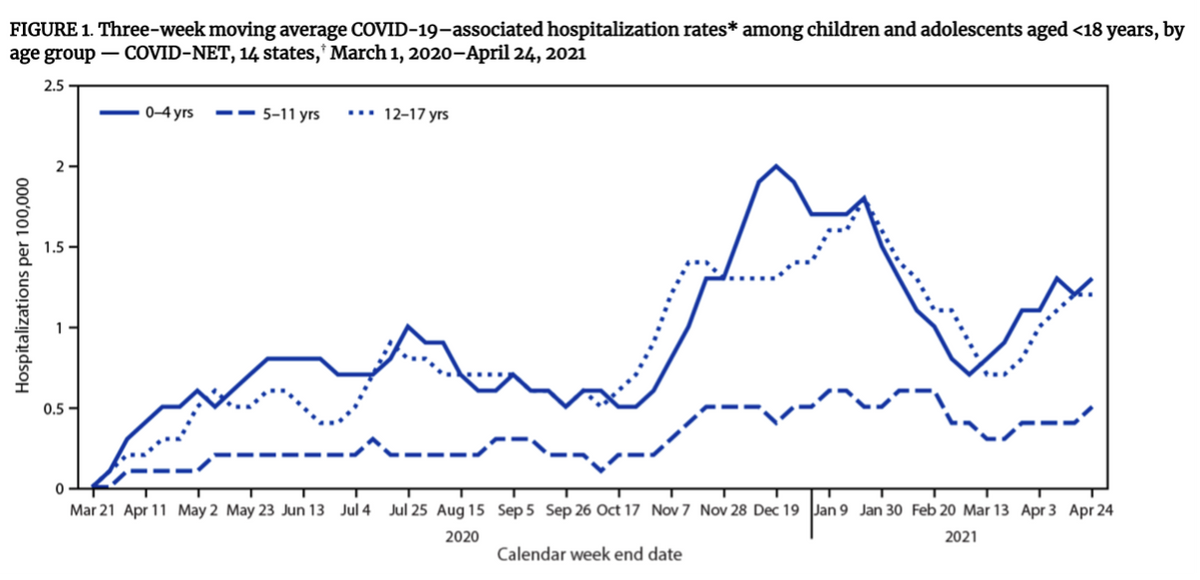
Manufacturing alarm at the very moment an age or other demographic cohort is targeted for vaccination has become a pattern for the CDC. On May 10, 2021, the FDA granted Emergency Use Authorization for the 12- to 15-year-old cohort to receive the Pfizer vaccine. On June 11, the CDC published a study in MMWR claiming to demonstrate rising hospitalization among this age group; widespread media coverage of the study quickly followed. But the absolute rates for this age group were, in reality, amazingly low: Less than 1.5 per 100,000, which was lower than they had been in the previous December. Meanwhile, a safety signal was being investigated—myocarditis, or inflammation of the heart muscle—which was more common after the second dose, and reported to be as frequent as 1 in 3,000-6,000, according to the Israeli Ministry of Health. Other countries became reluctant to push two doses within the standard 21- to 28-day timeline for these ages. By July, the U.K. had decided against pushing vaccines for this cohort, a decision that was walked back only slowly.
The CDC was undeterred, and in recent weeks the agency’s director has started to push for more doses at these ages. Against the advice of an FDA advisory committee, Rochelle Walensky has moved forward with recommending boosters for 12- to 15-year-olds. This view differs from WHO guidance and that of other countries, including Canada, which is not authorizing boosters for healthy adolescents aged 12-17. But when it comes to vaccination, the CDC has a single policy: All Americans should get three doses, regardless of age or medical conditions. This is not science as such, but science as political propaganda.
If that sounds like an exaggeration, consider a final example: the CDC’s near-total dismissal of natural immunity. Many other countries consider recovery from prior infection as a vaccination equivalent or better, an assumption that makes both medical and intuitive sense, but the CDC has steadfastly maintained that everyone needs the same number of vaccinations whether they have recovered from a COVID infection or not. This view is countered by data showing that vaccinating people who have recovered from COVID results in more severe adverse events than vaccinating people who have not had COVID.
In order to bolster the claim that people who have recovered from COVID benefit from vaccination as much as those who never had it, the CDC published a fatally flawed Kentucky-based analysis. The August 2021 study compared people who had contracted COVID twice against those who had it just once, and concluded that those who had it once were more likely to have had vaccination. But the study could have easily missed people who had two documented cases of COVID but might have had severe underlying medical conditions—such as immunosuppression—that predisposed them to multiple bouts of infection in a short period. In addition, people who had COVID once and then got vaccinated might not have sought further testing, believing themselves invulnerable to the virus. The study did not adequately address these biases. Months later, the CDC published a stronger, cohort study showing clearly that natural immunity was more robust than vaccine-induced immunity in preventing future COVID hospitalizations, and moreover, that people who survived infection were massively protected whether vaccinated or not.
But to listen to Walensky tell it, none of these complications even exist. On Dec. 10, 2021, she told ABC News that the CDC had seen no adverse events among vaccine recipients, and denied seeing any cases of myocarditis among vaccinated kids between 5 and 11. On that same day, however, data from her own agency showed the CDC was aware of at least eight cases of myocarditis within that age group, making her statement demonstrably false.
So why does the supposedly impartial CDC push weak or flawed studies to support the administration’s pandemic policy goals? The cynical answer is that the agency is not in fact impartial (and thus not sufficiently scientific), but captured by the country’s national political system. That answer has become harder to avoid. This is a precarious situation, as it undermines trust in federal agencies and naturally leads to a trust vacuum, in which Americans feel forced to cast about in a confused search for alternative sources of information.
Once that trust is broken, it’s not easily regained. One way out would be to reduce the CDC’s role in deciding policy, even during a pandemic. Expecting the executive agency tasked with conducting the science itself to also help formulate national policy—which must balance both scientific and political concerns and preferences—has proven a failure, because the temptation to produce flawed or misleading analysis is simply too great. In order to firewall policymaking from science, perhaps scientific agency directors shouldn’t be political appointees at all.
Ultimately, science is not a political sport. It is a method to ascertain truth in a chaotic, uncertain universe. Science itself is transcendent, and will outlast our current challenges no matter what we choose to believe. But the more it becomes subordinate to politics—the more it becomes a slogan rather than a method of discovery and understanding—the more impoverished we all become. The next decade will be critical as we face an increasingly existential question: Is science autonomous and sacred, or a branch of politics? I hope we choose wisely, but I fear the die is already cast.
Vinay Prasad is a hematologist-oncologist, associate professor of epidemiology and biostatistics at the University of California, San Francisco, and author of Malignant: How Bad Policy and Bad Evidence Harm People with Cancer.









